The most common adverse reactions include ulcerative stomatitis, leukopenia, nausea and abdominal distress. Although very rare, anaphylactic reactions to methotrexate have occurred. Others reported are eye irritation, malaise, undue fatigue, chills and fever, dizziness, loss of libido/impotence and decreased resistance to infection. In general, the incidence and severity of side effects are considered to be dose-related.
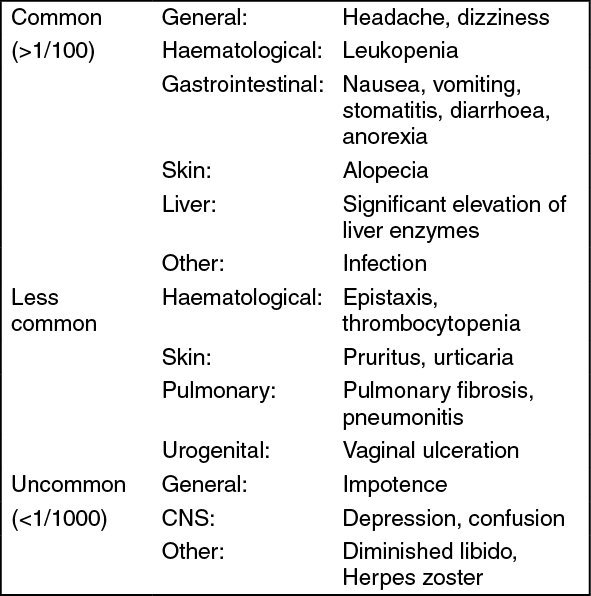
The incidence of the more frequent adverse reactions is as follows: See table.
 Click on icon to see table/diagram/image
Integument:
Click on icon to see table/diagram/image
Integument: Erythematous rashes, pruritus, urticaria, photosensitivity, pigmentary changes, alopecia, ecchymosis, telangiectasia, acne, furunculosis. Lesions of psoriasis may be aggravated by concomitant exposure to ultraviolet radiation. Skin ulceration has been reported in psoriatic patients. The recall phenomenon has been reported in both radiation and solar damaged skin.
Single cases of Stevens-Johnson-Syndrome and epidermal necrolysis have been reported.
Hematopoietic: Bone marrow depression is most frequently manifested by leukopenia, but thrombocytopenia, anaemia or any combination may occur. Infection or septicemia and haemorrhage from various sites may result. Hypogammaglobulinaemia has been reported.
Alimentary system: Mucositis (most frequently stomatitis, although gingivitis, pharyngitis and even enteritis, intestinal ulceration and bleeding) may occur. In rare cases the effect of methotrexate on the intestinal mucosa has led to malabsorption or toxic megacolon. Nausea, anorexia and vomiting and/or diarrhoea may also occur.
Hepatic: Reversible increase in transaminases occurs frequently. Hepatic toxicity resulting in significant elevations of liver enzymes, acute liver atrophy, necrosis, fatty metamorphosis, periportal fibrosis or cirrhosis or death may occur, usually following chronic administration.
Urogenital system: Renal failure and uraemia may follow methotrexate administration, usually in high doses. Vaginitis, vaginal ulcers, cystitis, haematuria and nephropathy have also been reported.
Pulmonary system: Infrequently an acute or chronic interstitial pneumonitis, often associated with blood eosinophilia, may occur and deaths have been reported. Acute pulmonary oedema has also been reported after oral and intrathecal use. Pulmonary fibrosis is rare. A syndrome consisting of pleuritic pain and pleural thickening has been reported following high doses.
In the treatment of rheumatoid arthritis: Methotrexate induced lung disease is a potentially serious adverse drug reaction which may occur acutely at any time during therapy. It is not always fully reversible. Pulmonary symptoms (especially a dry, non productive cough) may require interruption of treatment and careful investigation.
Central nervous system: Headaches, drowsiness and blurred vision have occurred. Following low doses of methotrexate, transient subtle cognitive dysfunction, mood alteration or unusual cranial sensations have been reported occasionally. Aphasia, paresis, hemiparesis, and convulsions have also occurred following administration of higher doses.
Adverse reactions particularly following intrathecal administration: Acute: chemical arachnoiditis manifested by headache, back or shoulder pain, nuchal rigidity, and fever.
Subacute: may include paresis (usually transient), paraplegia, nerve palsies and cerebellar dysfunction.
Chronic: leucoencephalopathy manifested by irritability, confusion, ataxia, spasticity, occasionally convulsions, dementia, somnolence, coma, and rarely death. There is evidence that the combined use of cranial radiation and intrathecal methotrexate increases the incidence of leucoencephalopathy.
Additional reactions related to or attributed to the use of methotrexate such as osteoporosis, abnormal (usually 'megaloblastic') red cell morphology, precipitation of diabetes, other metabolic changes and sudden death have been reported.
Carcinogenesis, mutagenesis, and impairment of fertility: Methotrexate has been reported to cause chromosomal damage to animal somatic cells and bone marrow cells in humans, these effects are transient and reversible. In patients treated with methotrexate, this may cause an increased risk of neoplasia (Lymphoma, usually reversible), but evidence is insufficient to permit conclusive evaluation. Methotrexate has been reported to cause impairment of fertility, oligospermia, menstrual dysfunction and amenorrhoea in humans, during and for a short period after cessation.
In addition, methotrexate causes embryotoxicity, abortion and foetal defects in humans. Therefore, the possible risks of effects on reproduction should be discussed with patients of child-bearing potential.



 Sign Out
Sign Out